Haemorrhoids, commonly known as piles, are primarily defined as the varicosities (enlarged or swollen veins) of the haemorrhoidal veins. This condition occurs in the lower part of the anus or rectum and is structurally similar to varicose veins found in the legs.
Studies carried out by various health institutes estimate that nearly 4.4% of the worldwide population suffers from haemorrhoids, with the peak incidence reported in adults between the ages of 45 and 65. In many cases, patients do not recognize the presence of symptoms and may not realize they have haemorrhoids until they progress.
Signs and Symptoms
The common signs and symptoms of haemorrhoids include:
- Painless bleeding during defecation (bowel movements)
- Mucous discharge after defecation
- Soreness, redness, and swelling around the anal region
- Itching or irritation in the anal area
- Discomfort and pain in the anal region
- Lumps around the anus
- Pain during bowel movements
What Causes Haemorrhoids?
While the exact root cause of haemorrhoids can sometimes be difficult to isolate, physicians identify several physiological and lifestyle factors that lead to the swelling or inflammation of these veins:
- Portal Hypertension: Increased pressure within the portal vein system.
- Chronic Constipation: Chronic straining during bowel movements significantly increases local venous pressure.
- Hereditary Predisposition: Inherited weakness of the venous walls.
- Venous Stasis in Pregnancy: Hormonal changes and pressure from the expanding uterus restrict blood return from the pelvis.
- Tumours of the Rectum: Obstructions that impede regular blood flow.
- Lifestyle Factors: Low-fibre diets, poor posture, obesity, and regular heavy weightlifting.
- History of Injury: Prior trauma to the anal region.
Additionally, as individuals pass the age of 50, the tissues that support the blood vessels of the lower abdomen and anal region naturally weaken, making older adults highly predisposed to straining and structural tissue laxity.
Classification: Types of Haemorrhoids
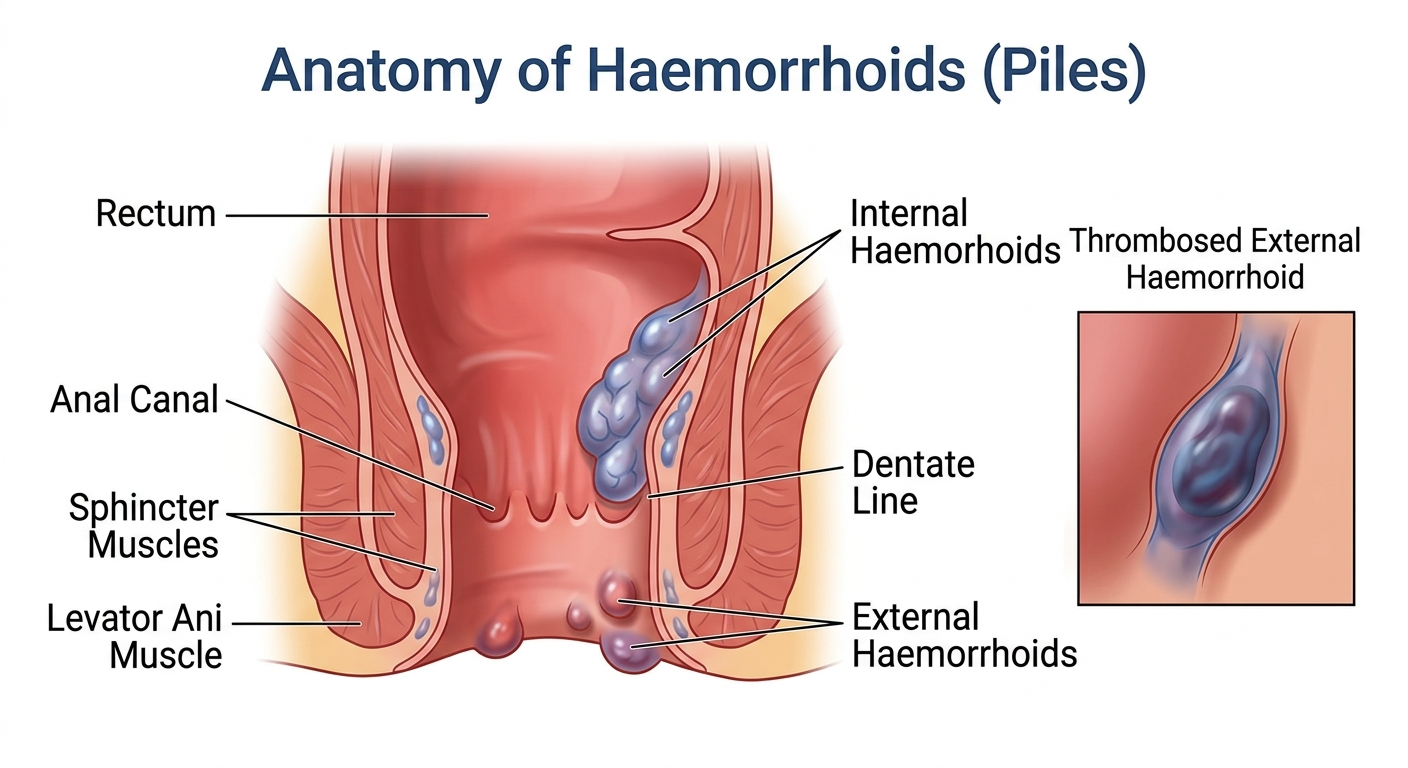
Haemorrhoids are broadly classified into two main types based on their structural location relative to the dentate line (the junction separating the upper and lower portions of the anal canal).
1. Internal Haemorrhoids
Internal haemorrhoids are located deep inside the rectum. They generally present with painless rectal bleeding because the upper rectum lacks pain receptors. While they rarely cause severe discomfort in their initial stages, prolonged straining can cause these veins to prolapse (protrude outside the rectum), temporarily losing their tendency to spontaneously return inside.
2. External Haemorrhoids
External haemorrhoids develop under the skin around the outer anal region. Because this area is rich in pain-sensing nerves, external haemorrhoids are associated with more intense itching and sharp pain. Occasionally, blood may pool and form a clot within these veins—a condition known as a thrombosed haemorrhoid—resulting in a hard, purple lump accompanied by sudden, severe pain and inflammation.
Potential Complications
If haemorrhoids are left untreated over a long period, they can progress to more severe medical manifestations:
- Anaemia: Chronic, severe blood loss during stools can exhaust the body’s iron stores, leading to iron-deficiency anaemia and systemic fatigue.
- Prolapse and Strangulation: When internal piles are severely prolapsed, they may become gripped by the internal anal sphincter. This restricts venous drainage, causing severe oedema (swelling), acute perianal pain, and potential tissue strangulation.
- Ulceration or Secondary Infection: Long-standing tissue inflammation can lead to open ulcers and bacterial infections in the anal region, increasing pain and discomfort.
- Thrombosis: Stasis of blood can lead to localized clotting, blocking venous drainage and causing acute, localized swelling.
- Anal Malignancy (Rare): While haemorrhoids themselves do not directly turn into cancer, advanced, untreated tissue damage or misdiagnosed chronic bleeding must be medically evaluated to rule out the uncontrolled, uncoordinated cell growth indicative of anal or colorectal cancer.
Diagnostic Procedures
While physical symptoms provide significant diagnostic clues, physicians use specific objective assessments to confirm the condition and rule out more serious gastrointestinal issues:
- Per Rectal (Digital) Examination: A manual exam performed to evaluate the lower rectum and rule out rectal carcinomas or other bleeding causes. Uncomplicated internal haemorrhoids cannot typically be felt via a digital exam unless they are severely thrombosed or fibrosed.
- Proctoscopy: The primary diagnostic procedure used to evaluate the anal cavity and rectum. Using a small, specialized tube called a proctoscope, physicians can directly visualize mucosal abnormalities, piles, or localized growths.
- Anoscopy, Sigmoidoscopy, and Colonoscopy: Advanced endoscopic evaluations used to rule out higher-level colorectal pathologies when bleeding occurs higher up in the digestive tract.
Dietary and Lifestyle Tips for Management
In mild cases, haemorrhoids can improve naturally through the body’s self-healing mechanisms without aggressive medical intervention. Implementing consistent lifestyle and dietary changes minimizes pressure on the pelvic blood vessels:
- Incorporate High-Fibre Dietary Sources: Consume plenty of fresh fruits, vegetables, whole grains, pulses, and seeds to bulk up the stool and eliminate chronic constipation.
- Maintain Hydration: Drink plenty of water and clear liquids throughout the day to keep stools soft and easy to pass.
- Limit Stimulants: Avoid alcohol and caffeine, as they can cause systemic dehydration and disrupt healthy bowel motility.
- Respond Promptly to Bodily Urges: Do not ignore or delay the urge to pass stools. Postponing bowel movements causes the colon to absorb excess water, making stools dry, hard, and painful to eliminate.
- Review Medications: Under medical guidance, minimize the use of pharmaceutical agents that list constipation as a primary side effect.
- Weight Optimization and Movement: Maintain a healthy weight to lower intra-abdominal pressure. Engage in regular, moderate aerobic exercise to stimulate healthy bowel peristalsis and regulate systemic blood pressure, avoiding prolonged sitting or heavy straining.
Treatment Options
Effective management depends heavily on the severity and clinical stage of the haemorrhoids.
1. Conventional Medical and Surgical Treatment
For early-stage haemorrhoids, conservative non-operative measures are standard. However, advanced or highly symptomatic cases generally require specialized medical interventions:
- Topical Therapeutics: Over-the-counter creams, protective ointments, and suppositories containing mild anti-inflammatories or local anaesthetics provide temporary symptomatic relief from burning and itching. Analgesics like acetaminophen or ibuprofen may be used to manage acute pain.
- Injection Sclerotherapy: A quick, typically painless outpatient procedure where a doctor injects a sclerosant solution (such as $5\%$ phenol in almond oil) into the submucosa layer. This induces aseptic thrombosis and subsequent fibrosis, safely shrinking early-stage internal haemorrhoids.
- Barron’s Rubber Band Ligation: A tiny elastic band is applied tightly over the base of the internal haemorrhoid. This cuts off its blood supply, causing the tissue to undergo local necrosis and drop off naturally within a few days, leaving behind a small scar.
- Surgical Intervention: For advanced, structural prolapses, a surgical haemorrhoidectomy or stapled haemorrhoidopexy may be required to physically excise or reposition the compromised vascular tissue.
2. Yoga and Naturopathy Interventions
Complementary therapies offer excellent non-invasive tools to reduce pelvic congestion, tone the pelvic floor muscles, and soothe inflamed local tissues.
- Warm Sitz Baths (Hydrotherapy): Soaking the perianal region in a clean tub or basin filled with comfortable, lukewarm water for 10 to 15 minutes, two to three times a day. This practice dramatically relieves sphincter spasms, increases localized blood circulation to accelerate tissue healing, reduces swelling, and maintains necessary local hygiene.
- Targeted Yoga Asanas: Incorporating specific yoga postures under professional guidance can alleviate abdominal and pelvic venous stasis:
- Viparita Karani (Legs-Up-the-Wall Pose): Promotes passive venous return from the lower limbs and pelvis back to the heart, minimizing blood pooling.
- Ashwini Mudra (Anal Lock Gesture): Involves rhythmic contraction and relaxation of the anal sphincter muscles, which strengthens the local pelvic floor and improves overall vascular tone.
- Pavanmuktasana (Wind-Relieving Pose): Gently massages the abdominal organs, improves digestive efficiency, and aids in relieving flatulence and chronic constipation.
3. Homoeopathic Approach
Homoeopathy aims to provide an individualized, holistic alternative to surgical intervention by evaluating the patient’s physical, mental, and emotional presentation. Medicines are selected based on the specific symptom patterns and underlying predisposing factors of the individual. Commonly used medicines by homoeopathic physicians to treat haemorrhoids include:
1. Homoeopathic Mother Tinctures (Q)
Mother tinctures are liquid extracts made directly from crude botanical or natural sources. In the treatment of piles, they are highly valued for their fast-acting, localized physiological effects. They can be taken internally (diluted in water) or applied topically as a soothing local application.
- Hamamelis Virginiana Q: Widely considered the premier remedy for bleeding piles. It acts directly on the coats of veins, causing them to contract and stop passive, dark-red bleeding. It rapidly relieves intense soreness, bruising, and the feeling of heaviness in the rectum.
- Aesculus Hippocastanum Q: Excellent for non-bleeding (blind) piles. It targets severe, sharp, shooting pains that radiate up the back or pelvis. It helps reduce the structural swelling of the haemorrhoidal veins and eases the sensation of “sticks” in the rectum.
- Millefolium Q: Specifically indicated when there is bright red, active, profuse bleeding from the piles without much pain. It acts as an efficient systemic haemostatic (agent that stops bleeding).
- Ficus Religiosa Q: A highly effective Indian botanical remedy used specifically for frequent, painful bleeding accompanied by hard stools.
- Ratanhia Q: Outstanding for relieving the excruciating, long-lasting burning pain that follows a bowel movement. It is often applied topically (diluted or formulated into an ointment) to soothe local fissures and severe anal itching.
- Mangifera Indica Q: A powerful styptic (agent that stops bleeding). It is specifically indicated for passive, bright red hemorrhoidal bleeding accompanied by marked localized soreness, a feeling of raw burning in the rectum, and mucous discharges. It helps tone relaxed mucous membranes.
- Carduus Marianus Q: The premier remedy when haemorrhoids are directly caused by liver disorders, pelvic congestion, or portal hypertension. It targets painful, bleeding piles associated with a sluggish liver, bilious digestive symptoms, and chronic constipation.
- Collinsonia Canadensis Q: Highly effective in tincture form for pelvic congestion. It targets dry, vascularly engorged internal piles with a persistent sensation of sharp sticks or sand in the rectum, especially during pregnancy.
- Aloe Socotrina Q: Used as a local or internal agent when piles protrude like a bunch of grapes. It addresses severe vascular engorgement, hot burning sensations in the anus, and stool incontinence due to weakened sphincter tone.
- Blumea Odorata Q: An excellent systemic anti-hemorrhagic remedy. It is highly useful for controlling active, profuse bleeding from internal piles where there is minimal localized pain but substantial blood loss.
- Cynodon Dactylon Q: A well-known hemostatic tincture used to check continuous, draining rectal bleeding during bowel movements. It assists in soothing inflamed local tissues.
2. Biochemic Tissue Salts (Schuessler Salts)
Biochemic therapy utilizes essential mineral salts to correct tissue deficiencies, restore venous elasticity, and improve bowel motility. For haemorrhoids, primary salts (typically in 6X or 12X potency) are used:
- Calcarea Fluorica: The Elasticity Restorer. The primary remedy for relaxed, dilated veins. It helps shrink enlarged external lumps and prevents structural prolapse.
- Ferrum Phosphoricum: The Inflammation Controller. Reduces throbbing pain, local redness, and manages bright red bleeding in the early stages.
- Kali Muriaticum: The Clot & Congestion Reliever. Helpful for swollen, thick, or clotted blood vessels (thrombosed piles) and mucous discharges.
- Natrum Muriaticum: The Moisture Regulator. Eases severe constipation by hydrating dry, hard stools that tear the anal lining.
3. Ultra-Diluted Homoeopathy Medicines
Ultra-diluted homoeopathy medicines (Used in 30, 200, 1M, 10M Potency) commonaly used by physicians include:
- Nux vomica: Frequently prescribed for individuals leading highly sedentary lives with a tendency toward a high-stress lifestyle, rich foods, or stimulants. It targets large, blind haemorrhoids presenting with a sharp stinging, burning, and constricted sensation in the rectum, alongside an ineffectual, frequent urge to pass stool.
- Lycopodium clavatum: Thought to be helpful for chronic, bleeding haemorrhoids that manifest as hard, bluish, congested vascular lumps containing large quantities of stagnant blood.
- Sulphur: A deep-acting constitutional remedy frequently utilized to address chronic haemorrhoidal issues intertwined with chronic constipation, portal stasis, and intense local redness, burning, and itching that worsens with warmth.
- Pulsatilla pratensis: Indicated when haemorrhoids stem from passive congestion or are secondary to dyspeptic, sluggish digestive issues. It is often considered clinically following or alternating with Aesculus.
- Graphites: A mineral-derived constitutional medicine utilized when hemorrhoidal veins present with severe soreness, burning, and deep stinging pains, particularly when the rectum feels as though it has lost its normal contractile power or is prone to painful fissures.
Note: Other remedies such as Ignatia, Capsicum, Arsenicum, Muriatic acid, Verbascum thapsus, Petroselinum and many more are also prescribed depending on the patient’s unique and peculiar symptoms.
Conclusion
Haemorrhoids are an incredibly common condition that can significantly disrupt an individual’s quality of life, yet they are highly preventable and manageable. Conventional medicine offers rapid symptomatic relief through topical treatments and minimally invasive procedures like band ligation or sclerotherapy. Long-term recovery often requires a multifaceted approach that includes integration of dietary fiber, maintaining optimal hydration, utilizing naturopathic tools like soothing warm sitz baths, practicing specific yoga postures to lower pelvic pressure, and exploring individualized holistic systems like homoeopathy that can address the root systemic causes.
Clinical Warning: Any instance of rectal bleeding should always be evaluated by a qualified medical professional to ensure an accurate diagnosis, rule out higher-level gastrointestinal pathologies, and establish a safe, supervised treatment plan.