Constipation is one of the most prevalent gastrointestinal disorders globally, affecting individuals of all age groups. In contemporary society, its incidence has risen sharply due to sedentary lifestyles, chronic stress, and a significant dietary shift toward ultra-processed, packaged, and fast foods. These modern dietary staples are highly refined and inherently deficient in essential micronutrients and dietary fiber.
Physiologically, constipation occurs when the normal motile functions of the digestive tract are disrupted. When a systemic or localized abnormality alters gastrointestinal transit time, a cascade of symptoms follows—ranging from localized abdominal discomfort to systemic manifestations like a loss of appetite, fatigue, and general malaise. Depending on the underlying etiology, constipation can manifest as an acute, short-term episode or develop into a debilitating, chronic condition that severely impacts an individual’s quality of life.
What is Constipation? The Physiological Mechanism
In clinical terms, constipation is defined as infrequent bowel movements (typically fewer than three times per week), difficulty or straining during defecation, a sensation of incomplete evacuation, or the passage of hard, dry stools that cause physical discomfort.
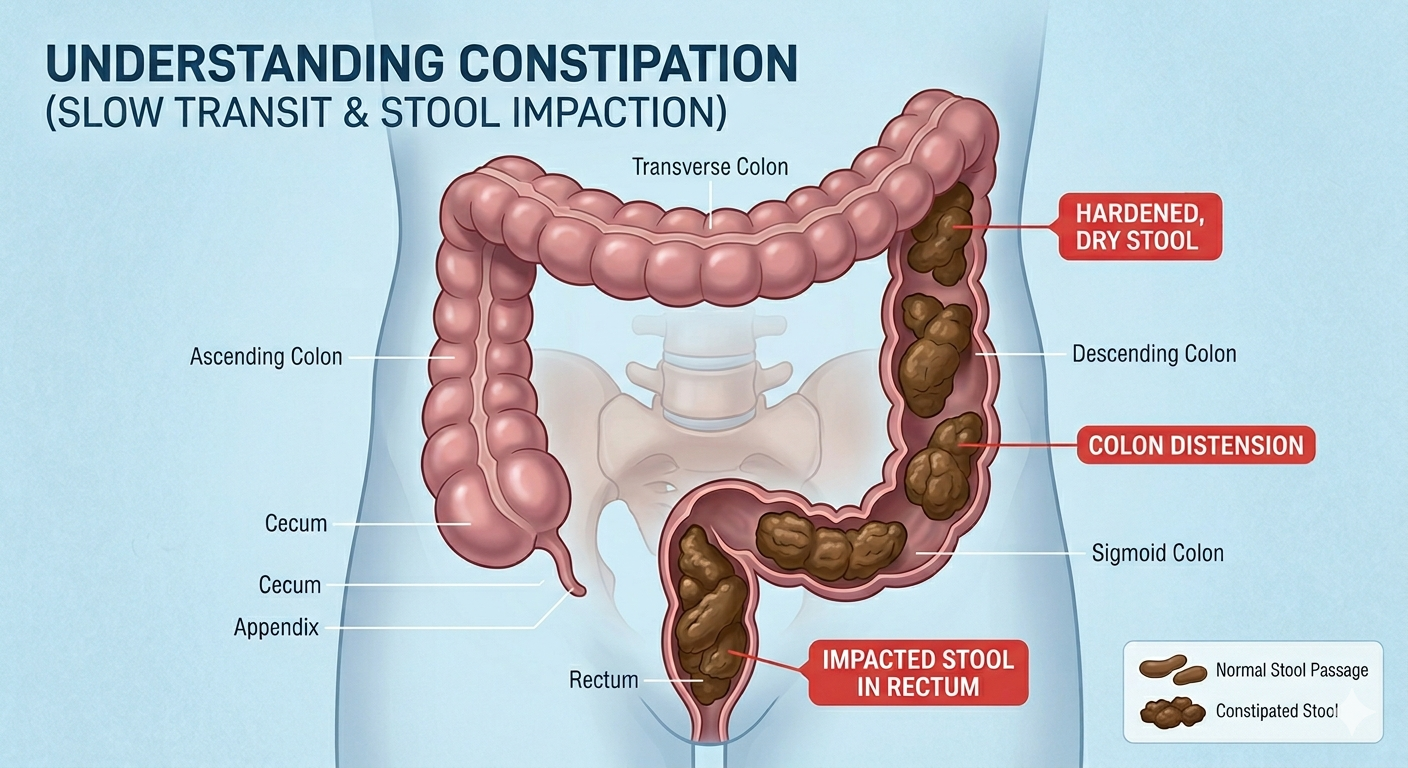
To understand how constipation develops, it is essential to look at the physiology of the large intestine (colon). The colon exhibits two primary types of muscular movements: segmental contractions (which mix the contents to facilitate the absorption of water and electrolytes) and peristaltic propulsions (mass movements that drive waste material forward). Under normal circumstances, the arrival of food in the stomach triggers the gastrocolic reflex, a neural signal that stimulates mass movements in the colon to push waste toward the rectum for evacuation.
When colon motility slows down or these movements are absent, fecal matter remains stationary in the large intestine for an abnormally prolonged period. The primary function of the colon’s mucosal lining is fluid absorption; therefore, the longer feces remain stagnant, the more water is extracted from them. This leaves the stool progressively harder, drier, and compacted within the rectal vault, requiring excessive intra-abdominal pressure (straining) to pass.
Signs & Symptoms
While a reduction in stool frequency is the most obvious sign, a comprehensive presentation of constipation includes both localized gastrointestinal and systemic symptoms:
- Difficulty and straining during bowel movements.
- Hard, dry, lumpy, or knotty stools (often classified as Type 1 or Type 2 on the Bristol Stool Chart).
- Abdominal pain, cramping, bloating, and generalized abdominal distension.
- A sensation of incomplete evacuation or an anorectal obstruction/blockage.
- Loss of appetite (anorexia) due to prolonged gastrointestinal retention.
- Foul breath (halitosis) and a furred or heavily coated tongue, arising from altered gut microbiota and delayed digestion.
- Inability to pass flatus (gas) comfortably, leading to trapped gas and severe flatulence.
- Rectal bleeding, usually presenting as streaks of bright red blood on the stool or toilet paper, caused by hard stools tearing the mucosal linings.
- General irritability, headache, and physical fatigue.
Causes of Constipation
The etiologies of constipation are multifactorial and can be classified into distinct clinical categories:
1. Dietary and Lifestyle Triggers
- Fiber Deficiency: A diet lacking in soluble and insoluble plant fibers reduces fecal bulk, slowing down peristalsis.
- Inadequate Hydration: Insufficient fluid intake forces the colon to absorb more water from the digestive waste, hardening the stool.
- Sedentary Habits: Physical inactivity reduces general metabolic rates and blunts natural intestinal motility.
- Disruption of Daily Hygiene & Routines: Traveling, changing time zones, or altering regular meal and sleep schedules can desynchronize the body’s natural circadian rhythms and bowel habits.
2. Pharmacological Causes (Drug-Induced Constipation)
Certain medications slow neuromuscular transmission within the gut wall:
- Opioids/Narcotics: Direct inhibition of enteric nervous system receptors.
- Antihypertensives: Particularly Calcium Channel Blockers (e.g., verapamil).
- Antidepressants: Tricyclic antidepressants possess strong anticholinergic properties that dry secretions and halt motility.
- Supplements: Iron and calcium supplements are widely known to cause stool compaction.
3. Neurogenic and Structural Intestinal Diseases
- Mechanical Obstructions: Colorectal tumors, strictures, or an internal collapse of the intestine (intussusception).
- Neurological Disorders: Conditions that disrupt the nerve pathways to the colon, such as a Stroke, Parkinson’s disease, Multiple Sclerosis, or Spinal Cord injuries.
- Systemic and Metabolic Conditions: Amyloidosis, Diabetes Mellitus, and Hypothyroidism (which profoundly slows down body metabolism).
- Motility Disorders: Conditions like Chronic Idiopathic Intestinal Pseudo-Obstruction (CIIP) or pelvic floor dyssynergia (incoordination of the muscles used during defecation).
4. Behavioral Causes
- Suppression of the Defecation Reflex: Regularly ignoring or delaying the urge to pass a bowel movement—often due to a lack of clean public facilities or busy schedules—gradually blunts the rectal nerves, causing the brain to lose responsiveness to the body’s natural signals.
5. Physiological Aging
- As individuals age, metabolic rates decline, muscle tone within the intestinal walls weakens, and structural pelvic floor changes occur, making older adults highly susceptible to chronic constipation.
Complications
If left untreated, severe or chronic constipation can lead to significant structural and functional complications within the anorectal region:
- Hemorrhoids (Piles): Swollen, inflamed veins in the rectum and anus caused by continuous straining. They can cause severe pain and frequent rectal hemorrhage (bleeding).
- Anal Fissures: Physical tearing and wearing of the delicate mucosal lining of the anus, resulting in sharp, burning pain during and after defecation.
- Rectal Prolapse: A condition where a small portion of the rectal mucous membrane protrudes outwards through the anus due to chronic intra-abdominal pressure.
- Fecal Impaction: A severe complication where a massive, hardened lump of dry stool becomes wedged securely in the rectum, completely resisting normal peristaltic clearance.
- Proctitis and Colitis: Localized inflammation of the rectal or colonic mucosa caused by the continuous chemical and mechanical irritation of stagnant fecal matter.
- Loss of Neuromuscular Reflexes: Over time, chronic distension of the rectum damages the localized nerve endings, leading to a permanent loss of the urge to defecate and a loss of function in the internal and external anal sphincters, occasionally leading to paradoxical fecal incontinence.
Diagnosis
While acute constipation is readily self-diagnosable based on individual symptoms, chronic or severe presentations require a systematic medical evaluation to rule out malignant or structural anomalies:
1. Clinical Evaluation
A physician conducts a detailed history regarding dietary habits, medication use, duration of symptoms, and a thorough digital rectal examination (DRE) to evaluate sphincter tone and check for impacted stool or structural masses.
2. Diagnostic Testing
- Blood Profiles: To screen for underlying metabolic conditions, such as checking Thyroid Stimulating Hormone (TSH) levels for hypothyroidism and serum calcium/glucose levels.
- Colonoscopy or Sigmoidoscopy: Direct visual examination of the interior mucosal walls of the large intestine using a flexible camera. This is crucial for detecting tumors, polyps, strictures, or inflammatory bowel diseases.
- Colonic Transit Studies: Tracking the movement of radiopaque markers or a wireless motility capsule through the GI tract via X-rays over several days to evaluate the speed of intestinal transit.
- Anorectal Manometry: A test evaluating the coordination of the pelvic floor muscles, anal sphincter pressures, and rectal sensitivity.
Conventional Medical Treatment
When lifestyle modifications prove insufficient, conventional medicine utilizes a tiered pharmacological approach tailored to the severity of the condition:
1. Laxatives
- Bulk-Forming Laxatives: (e.g., Psyllium husk, Methylcellulose). These act like natural fiber, absorbing water to create softer, bulkier stools that stimulate natural peristalsis. They are safest for long-term management.
- Osmotic Laxatives: (e.g., Polyethylene Glycol/PEG, Lactulose, Magnesium Hydroxide). These agents draw fluid into the bowel lumen from surrounding tissues, softening the stool and promoting easy transit.
- Stimulant Laxatives: (e.g., Senna, Bisacodyl). These actively trigger the rhythmic contractions of the intestinal smooth muscles. They provide fast relief but are reserved for short-term use to prevent dependency or bowel laziness.
- Stool Softeners: (e.g., Docusate Sodium). These act as surfactants, allowing water and fats to penetrate the hard fecal mass more easily.
2. Prokinetic and Secretagogue Agents
For severe, chronic idiopathic constipation, prescription medications like Lubiprostone or Linaclotide are used to accelerate intestinal fluid secretion and speed up transit times.
3. Manual Evacuation and Enemas
In cases of acute fecal impaction, targeted liquid enemas (such as saline or phosphate enemas) or physical manual fragmentation by a healthcare provider may be necessary to clear the rectal vault safely.
Diet, Nutrition, and Holistic Approaches
Dietary and Nutritional Management
Revising dietary intake is the foundational pillar of long-term bowel health. The objective is to increase fecal mass and maintain optimal intestinal hydration.
1. High-Fiber Fruits
- Prunes (Dried Plums): Exceptionally rich in insoluble fiber and containing natural sorbitol, a sugar alcohol that exerts a natural osmotic effect in the colon.
- Apples and Pears: These are loaded with pectin, a highly soluble fiber that undergoes fermentation in the gut to produce short-chain fatty acids, stimulating bowel contractions.
- Berries (Raspberries, Blackberries): These are packed with fibrous seeds that provide substantial bulk to the stool.
- Citrus Fruits (Oranges, Kiwis): These contain naringenin, a flavonoid that possesses a mild laxative effect, alongside high water and fiber content.
2. Fibrous Vegetables
- Cruciferous Vegetables: Broccoli, Brussels sprouts, and cabbage contain large amounts of insoluble fiber that speeds up waste transit through the intestines.
- Leafy Greens: Spinach and kale provide magnesium alongside fiber, which naturally helps relax the smooth muscles of the digestive tract.
- Root Vegetables: Carrots, sweet potatoes, and beets offer a balanced blend of soluble and insoluble fibers.
3. Hydration and Bulk Consumables
- Water: Consuming a minimum of 2 to 2.5 liters (approximately 8–10 glasses) of pure water daily is mandatory. Without adequate hydration, extra fiber can aggregate into a dense mass, inadvertently exacerbating constipation.
- Whole Grain Alternatives: Swapping refined flours for oats, brown rice, quinoa, and whole-wheat bran.
Holistic Approaches & Yoga
Physical movement mechanically massages internal organs and stimulates the enteric nervous system:
- Regular Exercise: Engaging in 30 minutes of daily moderate aerobic exercise, such as brisk walking or swimming, significantly increases intestinal peristalsis.
- Responding to Biological Signals: Never suppress the natural urge to pass stool. Establishing a consistent, unhurried routine (e.g., spending 10 minutes in the restroom shortly after breakfast) trains the body to reactivate its natural reflexes.
- Yoga Asanas: Specific yoga postures are highly effective at expanding and compressing the abdominal cavity to stimulate sluggish bowels. Some Yoga asanas are given below:
- Pavanmuktasana (Wind-Relieving Pose): Mechanically presses the ascending and descending colon, helping release trapped gases and promoting downward fecal movement.
- Malasana (Garland Pose/Deep Squat): The natural anatomical alignment of a deep squat relaxes the puborectalis muscle and straightens the anorectal angle, minimizing the need to strain.
- Ardha Matsyendrasana (Half Spinal Twist): Provides a deep intra-abdominal squeeze that stimulates the digestive tract and enhances localized blood circulation.
Homoeopathic Treatment for Constipation
Homoeopathy is a holistic system of medicine where treatments are highly individualized. Rather than prescribing a generic laxative, a homoeopathic physician selects a medicine based on the patient’s unique physical symptoms, constitutional makeup, and psychological state.
Important Clinical Directive: Homoeopathic medicines should be taken under the direct supervision and guidance of a qualified Homoeopathic Physician to ensure proper potency selection and dosage intervals.
Homoeopathy Medicines
I. Intestinal Atony & Paralytic Weakness (Lack of Expulsive Power)
These medicines target a complete lack of muscular tone or nervous response in the bowel wall, resulting in zero urge to defecate or an inability to expel even soft stools.
- Alumina
- Clinical Core: Complete rectal inactivity and mucosal dryness.
- Guiding Symptom: Even a soft, clay-like stool requires violent straining to pass because the rectum fills up without triggering an evacuative reflex.
- Target Patient: Frequently indicated for infants on artificial formula, sedentary individuals, and the elderly.
- Opium
- Clinical Core: Total neuromuscular paralysis and inertia of the bowel.
- Guiding Symptom: Absolute, chronic retention with no desire for stool whatsoever. Feces impact into small, round, black hard balls (like sheep dung).
- Target Patient: Ideal for post-operative constipation or bowel torpor following chronic laxative abuse.
- Silicea
- Clinical Core: Defective expulsive power due to pelvic floor and rectal weakness.
- Guiding Symptom: The classic “bashful stool”—the stool is partially expelled but slips back into the rectum because the muscles lack the physical grit to finish expulsion.
- Target Patient: Delicate, chilly individuals who tend to sweat heavily around the head when straining.
- Causticum
- Clinical Core: Localized paretic weakness of the muscular coat of the colon.
- Guiding Symptom: Stool is hard, tough, narrow, and shiny (as if greased). Evacuation is paradoxically easier when the patient stands up.
- Target Patient: Patients experiencing concurrent urinary weakness or those whose symptoms improve in damp, wet weather.
- Hydrastis canadensis
- Clinical Core: Chronic gastrointestinal atony and catarrhal mucous membrane inflammation.
- Guiding Symptom: Obstinate constipation dating back to the habitual abuse of over-the-counter purgatives. Stools are hard, lumpy, and entirely coated in thick, yellowish, tenacious mucus.
- Target Patient: Weak, debilitated individuals suffering from a chronic “sinking” feeling in the pit of the stomach.
II. Spasmodic & Irregular Intestinal Action (Incoordination)
These medicines apply when the bowel muscles are active but move in an uncoordinated, spasmodic, or reversed manner, often triggered by nervous stress or stimulant abuse.
- Nux vomica
- Clinical Core: Spasmodic, anti-peristaltic intestinal action.
- Guiding Symptom: Characterized by a frequent, irregular, and ineffectual urge for stool. The patient passes tiny amounts repeatedly but feels completely unsatisfied, as if more remains behind.
- Target Patient: Highly stressed, sedentary, or overworked individuals who abuse stimulants (coffee, alcohol, tobacco, or highly spiced food).
- Anacardium orientale
- Clinical Core: Loss of localized rectal reflexes paired with nervous gastrointestinal spasms.
- Guiding Symptom: An urgent desire for stool is felt, but the moment the patient sits on the toilet, the desire entirely vanishes. Accompanied by a sensation of a plug or foreign object wedged inside the rectum.
- Target Patient: Hypersensitive, anxious individuals whose gastrointestinal pain and constipation are temporarily relieved by eating a meal.
- Plumbum metallicum
- Clinical Core: Violent, spasmodic contraction of the intestinal smooth muscle.
- Guiding Symptom: Hard, lumpy, black spheres passed with a violent spasm of the anus. Marked by a sensation of a string pulling the abdomen and anus deeply inward toward the spine.
- Target Patient: Chronic, advanced cases accompanied by severe abdominal colic that is relieved by hard physical pressure.
III. Mucosal Dryness & Deficient Secretions
These medicines target the mucosal lining of the gut, where a lack of natural digestive fluids and lubrication causes the stool to become deeply compacted.
- Bryonia alba
- Clinical Core: Universal, acute dryness of the gastrointestinal mucous membranes.
- Guiding Symptom: Stools are large, hard, dry, knotty, and look dark or “as if burnt.” There is a total absence of the urge to pass stool, paired with an intense thirst for large quantities of cold water.
- Target Patient: Irritable, practical individuals whose symptoms are drastically worsened by the slightest physical movement.
- Natrum muriaticum
- Clinical Core: Systemic water imbalance resulting in localized dryness of the colon.
- Guiding Symptom: Stool is dry, hard, and crumbles at the anal margin, causing sharp, tearing pains and bleeding during defecation. Paired with a strong, insatiable craving for salt.
- Target Patient: Introverted, reserved individuals who suffer from concurrent bursting headaches.
IV. Venous Congestion & Structural Tissue Changes
These medicines are indicated when chronic constipation is tied to localized blood pooling (portal congestion), metabolic sluggishness, or painful structural lesions like fissures and hemorrhoids.
- Sulphur
- Clinical Core: Venous pooling and congestion within the portal system.
- Guiding Symptom: The passage of hard, dry stool causes intense, agonizing burning and intolerable itching at the anus, which appears visibly red, raw, and inflamed.
- Target Patient: Individuals prone to skin eruptions and flashes of heat, who alternate between chronic constipation and sudden morning diarrhea.
- Graphites
- Clinical Core: Sluggish glandular secretions tied to systemic metabolic delays.
- Guiding Symptom: Stools are unusually large lumps held together by gelatinous threads of mucus. Causes deep, painful cracks (fissures) around the anus that smart, sting, and bleed easily.
- Target Patient: Fleshy, chilly individuals prone to dry, cracked skin or chronic eczema.
- Sepia
- Clinical Core: Portal vein congestion leading to profound relaxation of the pelvic organs and uterine walls.
- Guiding Symptom: The defining sensation is feeling a heavy ball or weight wedged inside the rectum, which remains completely unaffected by passing a stool.
- Target Patient: Highly indicated for women during pregnancy, the postpartum phase, or menopause who experience a dragging-down sensation in the pelvis.
- Lycopodium clavatum
- Clinical Core: Hepatic (liver) insufficiency causing severe flatulent fermentation in the lower bowel.
- Guiding Symptom: The first part of the stool is hard, knotty, and difficult to expel, while the latter part is soft or loose. Accompanied by immense abdominal bloating and gas that is not relieved by passing flatus.
- Target Patient: Patients who crave warm food/sweets and experience a distinctive drop in energy between 4:00 PM and 8:00 PM.
Conclusion
Constipation is a multifaceted gastrointestinal disorder that extends far beyond simple irregularity; it is a direct reflection of our body’s interaction with our daily habits, diet, and neurological health. While the convenience of modern packaged foods and fast-paced schedules has made constipation a widespread modern ailment. It is highly manageable and preventable.
Addressing chronic constipation effectively requires a comprehensive, integrative strategy. Transitioning to a fiber-dense diet rich in fruits and vegetables, maintaining consistent daily hydration, respecting the body’s natural evacuation reflexes, and incorporating movement or yoga can successfully restore natural bowel motility for many individuals. When lifestyle adjustments alone are not enough, conventional options provide reliable structural relief, while individualized homoeopathic medicines offer a gentle, constitutional approach to stimulate the body’s natural digestive harmony. By understanding the underlying mechanics and addressing the root causes, individuals can successfully overcome constipation and protect their long-term gastrointestinal health.