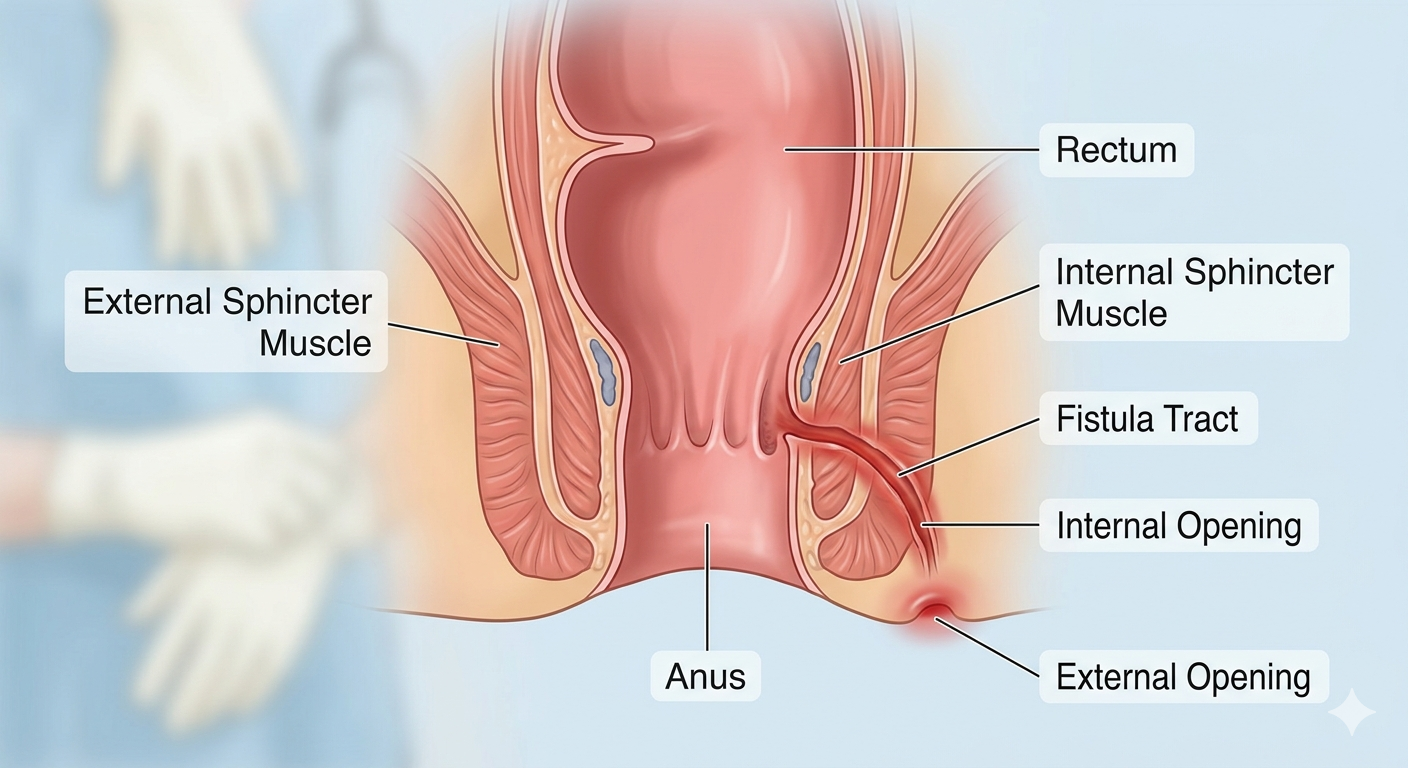
An anal fistula is an abnormal passage or tunnel that forms between the anal canal and the skin surrounding the anus. Additionally, fistulas can develop between internal organs. Examples include a rectovaginal fistula (an abnormal connection between the rectum and the vagina in females) and a rectovesical fistula (between the rectum and the urinary bladder in both male and females). In a rectovaginal fistula, gas and stool may inadvertently pass through the vagina, whereas in a rectovesical fistula, fecal matter or gas may enter the urinary bladder through the newly formed tunnel.
Signs and Symptoms
An anal fistula can present with a wide variety of symptoms, which commonly include:
- Perianal Abscess: A painful collection of pus in the tissue surrounding the anus.
- Foul-Smelling Discharge: Persistent leakage of offensive pus, fluid, or blood from the perianal opening.
- Skin Irritation: Itching, redness, and excoriation around the anal region.
- Pain and Swelling: Throbbing pain, soreness, and swelling that typically aggravate during sitting, physical activity, or immediately after a bowel movement.
- Systemic Symptoms: Fevers, chills, and a generalized feeling of being tired and unwell (malaise).
- Bleeding: Intermittent bloody discharge from the external fistula opening.
What Causes an Anal Fistula?
The development of an anal fistula is associated with a broad range of localized infections and underlying medical abnormalities. Key causes include:
- Frequent Anal Abscesses: The small mucus-secreting glands located just inside the anus can become clogged. This block leads to bacterial overgrowth and frequent abscess formation. In advanced stages, an unresolved abscess breaks through to the skin, creating a permanent fistula tract.
- Local Tissue Damage: Chronic injuries, trauma, or ruptures of the delicate tissues around the anal canal can cause cellular degeneration and subsequent tract formation.
- Chronic Gastrointestinal Infections: Inflammatory conditions affecting the digestive tract, such as Crohn’s disease and diverticulitis, significantly increase the risk of developing a fistula.
- Immune and Systemic Factors: Sexually transmitted infections (STIs), diabetes, localized ischemia (restricted blood supply), and a compromised immune system play a definitive role in compromising tissue healing.
- Surgical Complications: A fistula may sometimes arise as an unintended complication following major surgical procedures or instrumented deliveries (e.g., complex episiotomies or forceps delivery) in the pelvic and anorectal region.
Potential Complications
If left untreated or in complex chronic cases, an anal fistula can lead to several advanced health complications:
- Fistula Recurrence: Medical institutions estimate that anal fistulas recur in approximately 8% to 20% of patients following standard surgical interventions. The rate of recurrence depends heavily on the complexity of the fistula and the specific surgical technique utilized.
- Bowel Incontinence: This is the involuntary loss of control over bowel movements. During intricate surgeries, the anal sphincter muscles may accidentally become stretched or damaged, leading to varying degrees of incontinence.
- Persistent or Spreading Infection: If a fistula tract or associated abscess is not completely cleared or treated, the infection can become systemic or spread aggressively into surrounding deep pelvic tissues.
Who is at Risk?
Certain medical conditions and physiological factors increase a person’s vulnerability to developing an anal fistula:
- A History of Perianal Abscesses: Individuals who experience recurrent anal abscesses have a significantly higher risk of those abscesses progressing into chronic fistula tracts.
- Inflammatory Bowel Disease (IBD): Conditions like Crohn’s disease and ulcerative colitis cause chronic transmural inflammation of the bowel wall, directly accelerating fistula formation.
- Malignancy: Malignant tumors of the large intestine or rectum can infiltrate neighboring cells and structural tissues, causing necrotic breakdown and creating an abnormal passage.
- Trauma and Wounds: Deep injuries, unhealed perianal wounds, pelvic radiation therapy, tuberculosis, and HIV infection all heavily impair normal tissue repair, predisposing patients to fistulas.
How Anal Fistula Diagnosed?
Simple, superficial fistulas can often be diagnosed during a routine clinical examination by the visual presence of an external opening and associated clinical signs. However, for deep or complex tracks, doctors frequently conduct diagnostic procedures under anesthesia to avoid patient discomfort. Common diagnostic tools include:
- Anoscopy: An evaluation of the internal rectum and anal canal using a small, specialized tubular instrument called an anoscope. This allows the physician to visually inspect the internal mucosa for abnormalities.
- Fistula Probe: A thin, flexible instrument gently inserted through the external opening to trace the precise path and depth of the fistula channel.
- Computed Tomography (CT) Scan: A digital imaging examination that captures cross-sectional images from multiple angles to identify the location of fluid collections or secondary branches.
- Magnetic Resonance Imaging (MRI): A high-definition imaging modality that provides superior detail of the pelvic anatomy and soft tissues. It is widely considered as the gold standard diagnostic approach for confirming the complex anal fistula paths and mapping their relationship to the sphincter muscles.
How Anal Fistula Treated?
Conventional symptomatic management involves antibiotics to control active infection, analgesics for pain relief, and calcium channel blockers to reduce sphincter spasm. However, medication alone often fails to permanently seal the physical tract.
Consequently, surgical intervention is typically recommended as the definitive treatment of choice. Common surgical procedures include a fistulotomy (opening the tract to let it heal from the inside out), the seton technique (placing a surgical thread through the tract to drain infection), endoscopic ablation, or the application of fibrin glue to seal the channel.
Conservative Lifestyle & Management Advice
Alongside medical or surgical treatments, physicians advise implementing specific lifestyle modifications to promote optimal healing:
- Sitz Baths: Soaking the perianal region in a tub of warm water for 10 to 15 minutes, three to four times a day, to alleviate pain and maintain hygiene.
- Protective Padding: Wearing a soft, breathable pad over the area to absorb ongoing drainage while the tract heals.
- Dietary Adjustments: Consuming a diet enriched with high-fiber foods and drinking sufficient fluids to ensure soft stools and prevent straining.
- Activity Modification: Temporarily reducing strenuous daily activities and avoiding heavy exercises that put pressure on the pelvic floor.
Homoeopathic Approach and Common Medicines
Many patients explore holistic alternatives, and individual clinical case assessments indicate that homoeopathy can be supportive when tailored to specific symptom presentations. Homoeopathic medicines are prepared via potentization process from natural sources (plants, minerals, and organic compounds) and are selected based on individual symptom similarity. Common homoeopathic medicines used by the physicians include:
- Silicea Terra: Indicated when the fistula presents with copious, offensive, and purulent (pus-filled) discharge, often following a history of non-healing abscesses or hard nodules. It aims to reduce localized pain and assist the body in clearing cellular debris.
- Hepar Sulphuris Calcareum: Chosen for cases characterized by severe, throbbing pain where the perianal tissues are highly inflamed, swollen, and hypersensitive to even the slightest touch of clothing. Discharges are foul-smelling, and the patient may experience concurrent chills and irritability.
- Myristica Sebifera: Recognized for its historical association with suppurative processes, it is often utilized when there is deep inflammation of the skin and cellular tissues, often intended to encourage rapid drainage or resolution of an early-stage abscess.
- Calcarea Sulphurica: Indicated for individuals prone to frequent, recurrent abscesses where the discharge from the fistula opening is characteristically thick, yellow, and slow to heal.
- Hydrastis Canadensis: Particularly useful when the fistula is complicated by severe, chronic constipation. Stool passage causes sharp pain, and the local skin appears unhealthy, often accompanied by a distinct sinking sensation in the stomach.
- Thuja Occidentalis: Indicated when there is a sharp, pricking, needle-like pain inside an abscess or tract, occasionally accompanied by localized skin tags or warty overgrowths around the perianal region.
- Calcarea Phosphorica: Classically considered in homeopathic constitutional mapping when perianal complaints appear to alternate or coexist with respiratory vulnerabilities, or where bleeding occurs post-defecation in anemic individuals.
- Mercurius Solubilis: Selected when an anorectal abscess fails to heal properly and progresses to a chronic fistula. Symptoms typically feature thick, offensive pus accompanied by intense perianal itching that worsens at night and during rest.
- Lachesis Mutus: Indicated for septic-appearing conditions where the skin around the abscess or fistula looks bluish-purple, dark, or deeply congested, accompanied by foul discharge and a subjective relief of pain when soaking in warm water.
- Nitricum Acidum: Highly localized to bodily outlets (mucocutaneous junctions). It is indicated when there is a severe, splinter-like or pricking pain during and after passing stool, leaving the patient feeling exhausted and as though the rectum might tear.
In addition, Aesculus hippocastanum, Aloe Socotrina, Collinsonia canadensis, Pæonia officinalis, Ratanhia and many more medicines are also used by homoeopathic doctors to manage cases of anal fistula.
References
- National Center for Biotechnology Information (NCBI) PMC Article: PMC3160529
- IBD Relief – Complications of An Anal Fistula: IBD Relief Guide
- Wikipedia – Anal Fistula: Wikipedia Entry
- Winchester Hospital Health Library: Patient Resource
- NHS UK – Anal Fistula Conditions: NHS Guide