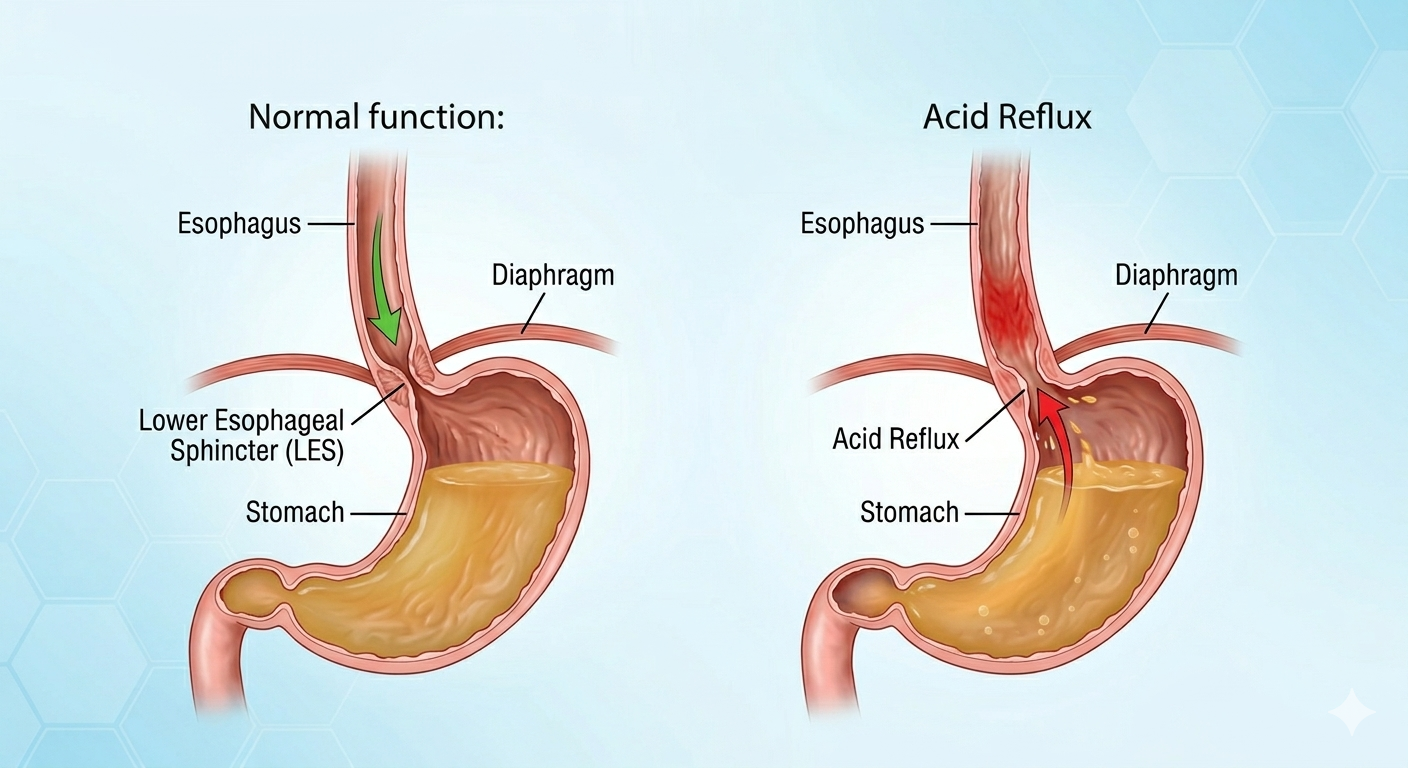
Gastroesophageal Reflux Disease (GERD) is a digestive disorder characterized by the regular regurgitation (bouncing back) of gastric contents into the esophagus—the muscular tube connecting the mouth to the stomach. While occasional reflux is common, particularly during stomach distension, belching, or burping, persistent reflux can damage the delicate esophageal lining.
Global healthcare studies estimate that roughly 20% of the world population suffers from GERD. With digestive disorders on the rise, increasing community awareness regarding dietary habits, lifestyle choices, and holistic wellness practices is vital to preventing complications like chronic heartburn, constipation, and diarrhea.
Signs & Symptoms
GERD presents with a wide range of mild to severe symptoms depending on the chronicity (long-term progression) of the condition:
- Heartburn: A burning sensation in the chest, usually after eating, which may be worse at night or when lying down.
- Nausea or vomiting
- Dysphagia and Odynophagia: Difficulty or pain during swallowing due to irritation of the esophageal mucosa (lining).
- Regurgitation: A sour or bitter taste in the mouth from backed-up food or acid.
- Flatulent Dyspepsia: Indigestion accompanied by gas, bloating, and abdominal discomfort.
- Sensation of a lump in the throat
- Offensive smell or bad breath originating from the stomach.
- Chest pain
Causes & Risk Factors
Medical professionals identify several anatomical, systemic, and environmental variables that contribute to the failure of the antireflux barrier:
- Acid Reflux Mechanics: Mechanical triggers often include overeating or lying down immediately after consuming food.
- Systemic and Structural Issues: Impaired esophageal peristalsis (the wave-like muscle movements that push food down), delayed gastric emptying, or an incompetent Lower Esophageal Sphincter (LES)—the muscular ring that acts as a valve between the esophagus and stomach.
- Hiatal Hernia: A medical condition where the upper part of the stomach bulges through the diaphragm into the chest cavity, preventing the LES from closing properly.
- Medications: Certain prescription drugs can relax the LES or irritate the gastric lining. Common culprits include antihistamines, sedatives, antidepressants, and asthma medications.
Populations at High Risk
- Obesity: Increased body weight elevates intra-abdominal pressure, physically forcing stomach contents upward through the LES.
- Pregnancy: Hormonal changes relax the smooth muscles of the LES, while the growing fetus physically increases pressure within the abdomen.
- Smokers: Nicotine relaxes the LES and reduces saliva production, which is necessary to neutralize stomach acid. Smoking also irritates both the respiratory and digestive tracts.
- Lifestyle Behaviors: Diets high in spicy, greasy, or fatty foods, chronic overeating, and erratic meal timings severely irritate the stomach lining.
Potential Complications
Left untreated, the prolonged exposure of the esophageal lining to corrosive stomach acid can lead to serious secondary medical issues:
- Esophagitis: Acute or chronic inflammation of the esophageal tissues.
- Esophageal Ulcers: Open sores that form when the protective mucus layer of the esophagus is eroded by acid, which can result in severe pain and internal bleeding.
- Esophageal Stricture: The narrowing of the esophagus due to scar tissue buildup from chronic irritation, making swallowing progressively harder.
- Barrett’s Esophagus: A condition where the normal squamous cells lining the lower esophagus are replaced by columnar cells similar to those in the intestines. This cellular change is a significant risk factor for developing esophageal cancer.
- Adenocarcinoma: Uncontrolled, uncoordinated cell growth forming a malignant tumor in the lower esophagus, which can lead to a complete blockage of the digestive pathway in advanced stages.
- Respiratory Aspiration: Refluxed acid entering the airways, causing chronic coughing, wheezing, or aspiration pneumonia.
Diagnostic Procedures
While physicians often diagnose GERD based on an analysis of a patient’s clinical signs and symptoms, specific medical procedures are utilized to confirm the diagnosis and assess tissue damage:
- Endoscopy: A procedure using a thin, flexible tube equipped with a camera to capture detailed images of the esophageal wall. It allows doctors to evaluate mucosal damage and easily perform tissue biopsies if abnormal cell growth is suspected.
- Esophagoscopy: Specifically evaluates the degree of tissue damage in the esophagus. Esophagitis is typically graded on a severity scale from 0 to 4. Physicians utilize either rigid or flexible esophagoscopes depending on the clinical requirement.
- Barium X-ray (Upper GI Series): A radiographic examination where the patient swallows a contrast liquid (barium) to illuminate structural abnormalities like hiatal hernias, strictures, or severe ulcers on an X-ray.
- Ambulatory Acid pH Test: Monitors the precise acid levels inside the esophagus over a 24-hour period to correlate symptoms with actual reflux events.
- Esophageal Impedance Test: Measures the physical movement of liquids and gases through the esophagus, helping diagnose non-acid reflux presentations.
Diet, Nutrition & Lifestyle Adjustments
Strategic nutritional changes directly reduce the workload on your stomach and prevent the lower esophageal sphincter from relaxing unnecessarily.
Dietary Recommendations
- Foods to Include: Focus on highly alkaline, low-fat foods. Whole grains (oatmeal, brown rice), green vegetables (broccoli, asparagus, celery), non-citrus fruits (bananas, melons, apples), and lean proteins (chicken breast, egg whites, fish) naturally absorb stomach acid and digest easily.
- Foods to Avoid: Strictly limit high-fat or greasy items, which delay stomach emptying. Avoid chocolate, peppermint, garlic, onions, and heavy spices, all of which naturally relax the muscle tone of the LES.
- Portion Control: Consuming three large meals distends the stomach wall and increases upward mechanical pressure. Switch to 5–6 small meals distributed evenly throughout the day.
- Hydration: Drink plenty of water between meals rather than during them to prevent the stomach from overfilling.
Preventive Home Tips
- Elevate the Head of the Bed: Raise the headrest of your bed by 6 to 9 inches using blocks under the bedposts or a firm wedge pillow. Relying on stackable regular pillows only bends your neck, whereas a steady incline keeps stomach acid down through natural gravity.
- The 3-Hour Buffer Rule: Never lie down flat within 3 hours of eating. Allow your stomach adequate time to empty its contents into the small intestine while you are still upright.
- Sleep on Your Left Side: Clinical studies show that sleeping on your left side positions the junction between your stomach and esophagus above the level of gastric acid, reducing active reflux incidents at night.
- Avoid Abdominal Constriction: Keep your wardrobe loose. Tight-fitting belts, corsets, or high-waisted pants apply physical compression to your abdomen, squeezing acid past the LES.
Yogic Practices & Internal Cleaning Techniques
Yoga offers excellent therapeutic benefits for the digestive system by reducing systemic stress (a major trigger for acid oversecretion) and strengthening the diaphragm, which physically supports the lower esophageal sphincter.
Important Note on Timing: Never practice active yoga asanas, deep abdominal breathing, or cleansing techniques on a full stomach. Asanas should be performed 3 to 4 hours after a heavy meal, while traditional internal purification practices must strictly be done first thing in the morning on an empty stomach.
Traditional Yogic Cleansing (Shatkarma)
Vaman Kriya (Kunjal Kriya) purification practice.
- Vaman Kriya / Kunjal Kriya (Therapeutic Vomiting): This is a traditional Dhauti (cleansing) technique practiced first thing in the morning on an completely empty stomach. The practitioner drinks 4 to 6 glasses of lukewarm, lightly salted water rapidly until the stomach is completely full, and then stimulates the back of the throat with the fingers to induce a smooth, voluntary reflex that expels the water.
- How it helps GERD: It washes away stagnant residual acids, stubborn bile, and excess mucus from the stomach lining, resetting the stomach’s pH and neutralizing hyperacidity. It also helps tone and strengthen the lower esophageal sphincter over time.
- Crucial Warning: Vaman Kriya should only be learned and practiced under the direct guidance of an experienced yoga expert or yoga therapist. It is strictly contraindicated for individuals suffering from severe esophageal ulcers, active internal bleeding, hernia, or severe hypertension.
Asanas & Breathwork
- Vajrasana (Thunderbolt Pose): The only yoga pose recommended immediately after a meal. Kneeling on your shins for 5–10 minutes alters blood flow patterns, focusing circulation directly in the abdominal region to enhance digestion and alleviate bloating.
- Pawanmuktasana (Wind-Relieving Pose): Gently compresses the digestive organs to release trapped gas and intestinal pressure, preventing the lower abdomen from bloating upward against the stomach.
- Shavasana (Corpse Pose): Deep relaxation dampens down the sympathetic (“fight-or-flight”) nervous system, lowering stress-induced gastric acid production.
- Pranayama (Controlled Breathing): Gentle, steady practices like Anulom Vilom (Alternate Nostril Breathing) bring balance to the nervous system. Avoid aggressive abdominal-churning exercises like Kapalbhati or Bhastrika if your GERD is highly active, as aggressive bouncing can mechanically push acid upward.
Treatment Approaches
1. Conventional Medicine Approach
Conventional management heavily relies on medications that lower acid production or neutralize existing stomach acid. These include:
- Antacids: Over-the-counter options (such as Mylanta or Rolaids) that neutralize stomach acid for rapid, temporary relief.
- H2-Receptor Blockers: Medications (such as cimetidine or nizatidine) that turn down acid production to allow the esophageal lining time to heal.
When lifestyle modifications and aggressive medical therapies fail to provide relief, surgical interventions (such as fundoplication) are considered to mechanically strengthen the LES.
2. Homoeopathy Medicine Approach
Homoeopathy physician views health as a state of dynamic equilibrium maintained by an underlying organizing energy—traditionally termed as Vital Force. When this vital force is disrupted by environmental stressors, genetic predispositions, poor diet, or psychological conflict, it expresses its internal disharmony through a unique constellation of physical, mental, and emotional signs. Commonly recommended homoeopathic medicines for gastric complaints include:
- Arsenicum Album: Indicated for deep-acting gastric complaints marked by intense, burning pain in the epigastric region that feels “like fire.” It is often chosen when gastric irritability manifests as persistent nausea, vomiting, waterbrash (sudden hyper-salivation mixed with acid), and a total loss of appetite.
- Nux Vomica: The primary remedy for gastric complaints stemming from a sedentary lifestyle, high stress, or dietary indulgence. It addresses cases where the stomach feels heavily distended and sensitive to external pressure. Food feels like a “heavy stone” sitting in the stomach, accompanied by acid eructations. The classic indicator is a persistent, frustrating feeling that vomiting would bring relief, but the urge remains unfulfilled.
- Iris Versicolor: Known as one of the preeminent “sour” remedies due to marked hyperacidity. It acts directly upon the gastrointestinal mucous membranes and digestive glands, making it a frequent choice for dyspepsia, severe gastric burning, gastric ulcers, and duodenitis.
- Phosphorus: A constitutional remedy traditionally adapted to tall, slender individuals. It targets gastric symptoms like stomach ulceration and the vomiting of sour, bitter mucus. Key indicators include a sensation of hard pressure in the pit of the stomach and cutting pains that are temporarily relieved by drinking cold liquids. It is also utilized to mitigate the chronic gastric side effects of long-term alcohol consumption.
- Pulsatilla: Often selected for individuals who experience slow digestion and frequent vomiting spells after eating rich, fatty, or greasy foods. Symptoms include a distinct gnawing distress in the stomach pit that mimics an ulcerated sensation.
- Natrium Phosphoricum: A primary biochemical remedy for chronic dyspepsia characterized by systemic acidity. This acid state manifests globally as a sour taste in the mouth, sour eructations, sour vomiting, and even an acidic smell to the patient’s perspiration.
- Robinia: Highly recommended for excessive gastric acid hypersecretion. Food turns sour almost immediately upon entering the stomach, leading to intensely sour burping and the painful vomiting of liquid, highly acidic ingesta.
- Carbo Vegetabilis: Indicated for severe upper abdominal bloating, flatulence, and constant gas. The patient experiences frequent, uncomfortable eructations of wind and gurgling colic. It is primarily used when symptoms are the direct result of overindulgence in rich, heavy, or indigestible foods.
Note: Other homoeopathic remedies—such as Calcarea Carbonica, Sulphuric Acid, Antimonium Crudum, Bryonia Alba, Cinchona, Colocynthis,Magnesium Phosphorica and many more may also prescribed on basis of patient’s unique, peculiar presentation.
Conclusion
Gastroesophageal Reflux Disease (GERD) is far more than a simple case of temporary indigestion; it is a complex, multifaceted disorder that impacts nearly a fifth of the world’s population. As detailed above, the condition progresses through a combination of anatomical factors, dietary choices, and heightened lifestyle stress. Leaving the esophageal wall unprotected against regular acid exposure risks severe, long-term complications ranging from strictures and regular bleeding to cellular transformations like Barrett’s Esophagus.
A truly effective, long-term resolution for GERD requires looking beyond temporary symptom suppression. By combining early clinical diagnostic confirmation with proactive dietary changes, simple preventive home strategies, therapeutic yogic asanas, and internal purification methods like Vaman Kriya, patients can target the true root causes of acid backup. Whether managed through conventional medical therapies or individualized holistic approaches like homeopathy, prioritizing daily lifestyle awareness remains the core foundation to protecting digestive health and achieving lasting systemic relief.