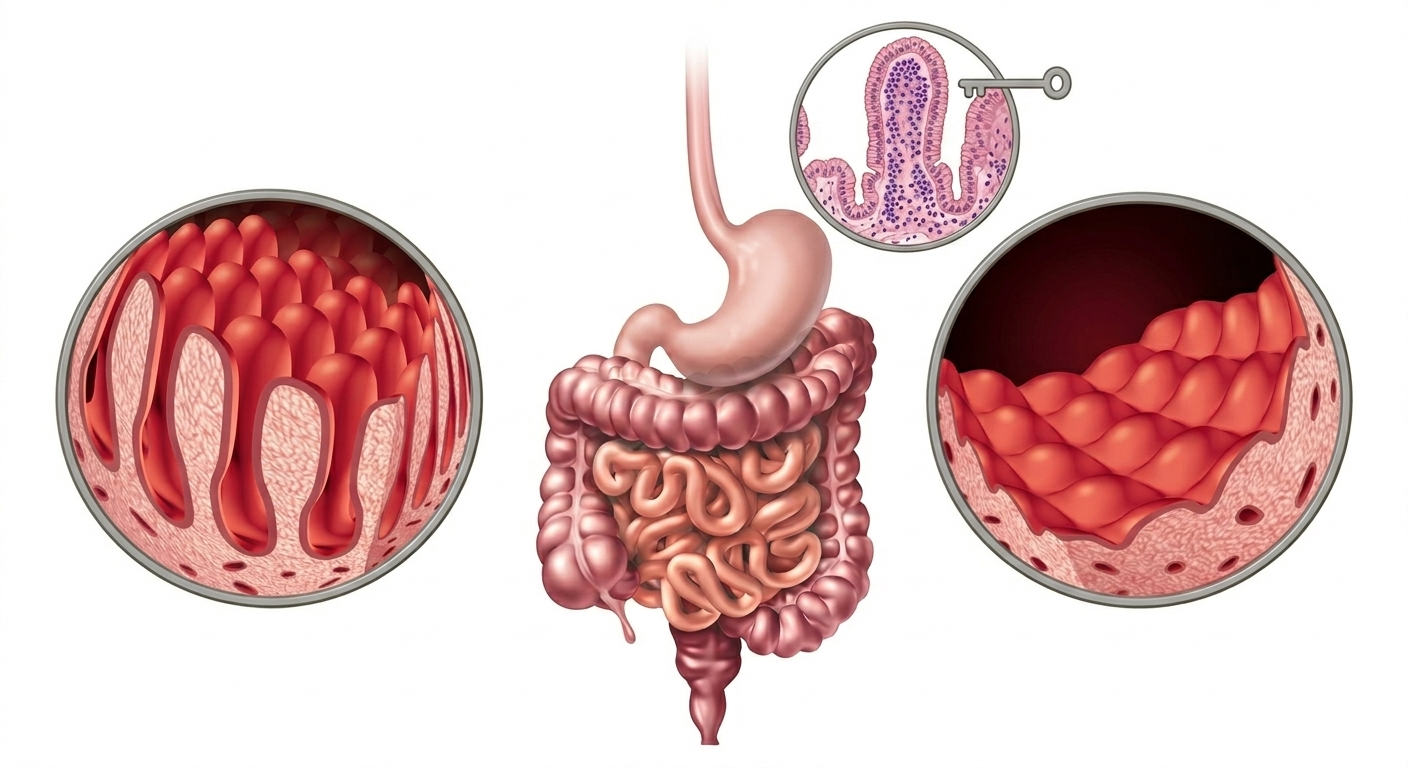
Celiac disease is an autoimmune disorder characterized by damage to the mucosa and atrophy of the villi in the small intestine, resulting in impaired digestion and nutrient absorption. It is also known as gluten-sensitive enteropathy, celiac sprue, and non-tropical sprue. Three primary cereals contain gluten that is harmful to celiac patients are: wheat, rye, and barley.
The epidemiology of celiac disease has changed rapidly over the last half-century. Health institutions estimate that seven out of eight people with celiac disease remain undiagnosed, often dismissing their symptoms as normal, temporary bodily derangements. Patients frequently go undiagnosed due to a lack of community awareness, socioeconomic factors, and the limited availability of advanced endoscopy services in public hospitals.
Signs and Symptoms
Celiac disease is often more readily diagnosed in children than in adults, with a classic peak age of diagnosis between 6 and 24 months as new foods are introduced. However, it can manifest at any age. Symptomatology varies greatly from person to person and shifts over time. Common presentations include:
- Diarrhea: Frequent, loose, or watery stools.
- Steatorrhea: Foul-smelling, pale, bulky stools caused by fat malabsorption (often compounded by a secondary deficiency of pancreatic lipase).
- Abdominal Pain: Cramping, bloating, and general distress.
- Weight Loss: Inability to maintain or gain weight despite adequate food intake.
- Behavioral Changes: Irritability in children; depression or anxiety in adults.
- Distended Abdomen: Visible swelling or bloating of the stomach.
- Tiredness and Fatigue: Chronic exhaustion resulting from systemic inflammation and anemia.
What Causes Celiac Disease?
Celiac disease is an autoimmune condition that occurs in genetically susceptible individuals. It is triggered by the ingestion of gluten and associated plant storage proteins found in wheat, rye, and barley. When gluten is consumed, it triggers an abnormal immune response that targets the lining of the small intestine, leading to the flattening of the villi and progressive nutrient malabsorption. Genetic susceptibility is strongly linked to specific human leukocyte antigen (HLA) class II regions, primarily the HLA-DQ2 and HLA-DQ8 haplotypes (historically referred to in relation to DR3 and DR4).
Histological Classification (The Marsh Criteria)
The standard histological classification of celiac disease is given by Marsh. It organizes the disease into distinct, progressive stages based on the microscopic appearance of the intestinal tissue:
- Type 0 (Pre-infiltrative stage): The intestinal lining appears completely normal under a microscope, even if the patient has positive blood tests (serological criteria).
- Type 1 (Infiltrative stage): Characterized by a significantly increased number of intraepithelial lymphocytes (IELs) within the bowel mucosa, though the structure of the villi remains intact. This stage is also monitored in patients undergoing a gluten-free diet assessment.
- Type 2 (Hyperplastic stage): Characterized by both an increase in intraepithelial lymphocytes and an enlargement (hyperplasia) of the intestinal crypts, alongside shortening of the villi. This stage is rare but is occasionally observed in patients who also suffer from dermatitis herpetiformis (a blistering skin manifestation of gluten sensitivity).
- Type 3 (Destructive stage): Characterized by progressive, structural villous atrophy. It is sub-classified into partial, subtotal, or total villous atrophy. While extensive structural damage takes time to reverse, most cases can be successfully managed and healed over time with strict therapeutic intervention.
Complications
If left untreated or poorly managed, celiac disease can lead to several severe complications:
- Refractory Celiac Disease: Formally known as “refractory sprue,” this is a rare and severe form of the disease where intestinal damage and malabsorption persist despite a strict, verified gluten-free diet for over 12 months. It most commonly occurs in older adults and is divided into Type I and Type II based on the clonal profile of intraepithelial lymphocytes.
- Malnutrition: Chronic malabsorption leads to profound deficiencies in essential vitamins and minerals (such as iron, folate, vitamin B12, and fat-soluble vitamins), accompanied by severe weight loss.
- Bone Weakening: Malabsorption of calcium and vitamin D often leads to early-onset osteopenia or osteoporosis, resulting in bone deformities and increased fracture risks.
- Infertility and Reproductive Issues: Chronic malnutrition and systemic inflammation can lead to unexplained infertility, recurrent miscarriages, and low birth weight in newborns.
- Secondary Lactose Intolerance: Because the enzyme lactase is produced at the tips of the intestinal villi, extensive damage to the intestinal wall can temporarily strip the body’s ability to digest dairy products, triggering diarrhea and abdominal pain.
- Malignancy and Neurological Disorders: Long-term untreated celiac disease elevates the risk of developing intestinal cancers (such as enteropathy-associated T-cell lymphoma). It can also cause neurological issues like peripheral neuropathy and ataxia (loss of balance).
Diagnosis
A definitive diagnosis relies on a combination of clinical assessment, blood testing, and tissue evaluation:
- Serological Tests: Blood tests measuring specific autoantibodies are highly accurate. Anti-tissue transglutaminase IgA (tTG-IgA) and Anti-endomysial IgA (EMA-IgA) antibodies approach a 95% sensitivity and specificity rate in both children and adults.
- Endoscopic Biopsies: Visual inspection and collection of tissue samples from the duodenum via an upper endoscopy remain the diagnostic gold standard. Taking multiple biopsies from different areas reduces the risk of a false-negative result due to patchy tissue damage.
- Dietary Response: Documenting clear clinical and laboratory improvement after adopting a strict gluten-free diet—particularly the eventual disappearance of celiac-specific antibodies—confirms the diagnosis.
Approaches to Treatment
1. The Conventional Medical Approach
The primary, universally accepted conventional treatment for celiac disease is a strict, lifelong adherence to a gluten-free diet (GFD).
- Dietary Elimination: Patients must completely avoid all foods, beverages, medications, and cosmetic products containing wheat, rye, barley, and their derivatives (such as spelt, kamut, and malt).
- Symptom Resolution: In highly symptomatic patients, gastrointestinal relief is achieved relatively quickly. Symptoms typically begin to resolve within a few weeks in children, while adults may take several months to see full symptomatic recovery and mucosal healing.
- Nutritional Supplementation: Conventional physicians frequently prescribe targeted iron, calcium, vitamin D, and B-complex supplements during the initial recovery phase to correct underlying deficiencies.
- Monitoring: Regular follow-up appointments, repeat serology testing, and occasional follow-up biopsies ensure that the intestine is healing and that gluten is successfully missing from the diet.
2. The Homeopathic Approach
Homeopathy views celiac disease as a systemic, constitutional imbalance rather than an isolated intestinal issue. It aims to offer safe, gentle, and complementary support tailored to the specific symptomatic profile of the individual.
Homeopathic prescriptions are selected based on the “totality of symptoms,” taking into account the patient’s physical, mental, and emotional state. In advanced stages (such as the hyperplastic or destructive stages), remedies may be approached through miasmatic classification:
- Psora: Associated with underlying functional disturbances, sensitivities, and inflammation.
- Sycosis: Associated with hyperplastic changes and overgrowth (e.g., crypt hyperplasia).
- Syphilis: Associated with structural destruction and tissue atrophy (e.g., villous atrophy).
Common Homoeopathic Medicines
The following medicines are traditionally used in homoeopathic practice based on specific symptom presentations:
- Natrum Sulphuricum: Often utilized within Schuessler’s tissue salt therapy framework to help regulate fluid balance and digestive secretions. It is indicated for chronic symptoms such as sudden, watery, yellowish diarrhea, involuntary stools, and burning sensations in the abdomen.
- Cinchona Officinalis (China): Widely used for gastric distress characterized by severe bloating, gas, and painless, exhausting yellow diarrhea triggered by specific dietary items. It is frequently considered when a patient feels weak from a loss of vital fluids.
- Carbo Vegetabilis: Suited for chronic, sluggish digestive states. It is indicated when there is severe abdominal pain, excessive accumulation of fetid gas, and a constant sensation of fullness, particularly in individuals who feel weak and fatigued.
- Kali Carbonicum: A notable remedy in homeopathic materia medica for profound flatulence and upper abdominal distress. It is considered when a patient experiences a sensation of a “lump” or intense pressure in the pit of the stomach, accompanied by sharp, cutting pains that worsen after consuming cold liquids.
- Lycopodium Clavatum: Indicated when the patient suffers from weak digestion, a constant sense of fermentation in the upper-left abdomen (as if “yeast is working”), and bloating that typically aggravates between 4:00 PM and 8:00 PM.
- Arsenicum Album: Indicated when celiac disease causes severe weight loss, exhaustion, and intense anxiety. The patient often cannot tolerate the sight or smell of food, and suffers from burning abdominal pains and watery, acrid diarrhea.
Note: Other constitutional remedies like Calcarea Phosphorica, Phosphorus, Thuja Occidentalis, Sulphur, Silicea, Nux Vomica and many more may also be selected by a qualified practitioner based on individual characteristics.
Conclusion
Celiac disease is a serious, global autoimmune condition driven by an inherited genetic susceptibility to gluten, a protein complex found in wheat, rye, and barley. Millions worldwide suffer from its multi-systemic effects, yet a significant portion of the population remains undiagnosed.
The cornerstone of modern medical management remains the strict, lifelong elimination of gluten from the diet, which successfully halts immune-mediated damage and allows the intestinal mucosa to recover. Concurrently, holistic approaches like homoeopathy seek to complement this management by focusing on constitutional vitality and symptomatic relief, aiming to restore internal equilibrium at the physical, emotional, and energetic levels. Managing celiac disease effectively requires a proactive approach combining early diagnostic screening, rigorous dietary discipline, and personalized medical guidance.